Dental and Surgical Care For Cleft Lip and Palate
Cleft Lip and Cleft Palate
A cleft lip and cleft palate are openings in a baby’s upper lip or roof of the mouth (palate). They’re congenital abnormalities (birth defects) that form while a fetus develops in the uterus. Cleft lips and cleft palates happen when tissues of the upper lip and roof of the mouth don’t join together properly during fetal development. Surgery is required to repair cleft lip and cleft palate.
What is cleft lip?
Our lips form between four and seven weeks of pregnancy. Tissues from each side of our head join together at the center of the face to make our lips and mouth. A cleft lip happens when the tissues that make the lips don’t join completely. As a result, an opening or gap forms between the two sides of the upper lip. The cleft can range from a small indentation to a large gap that reaches the nose. This separation can include the gums or the palate (roof of the mouth).
What is cleft palate?
The roof of your mouth (palate) forms between six and nine weeks of pregnancy. A cleft palate is a split or opening in the roof of your mouth that forms during fetal development. A cleft palate can include the hard palate (the bony front portion of the roof of the mouth) or the soft palate (the soft back portion of the roof of the mouth).
Cleft lip and cleft palate can occur on one or both sides of the mouth. Because the lip and the palate develop separately, it’s possible to have a:
- Cleft lip without a cleft palate.
- Cleft palate without a cleft lip.
- Both a cleft lip and cleft palate (the most frequently occurring disorder).
How will a cleft lip or cleft palate affect my baby?
Babies born with a cleft lip or cleft palate may have difficulties eating (both from the breast and a bottle). They may also have trouble speaking, and they often have fluid behind their eardrum that can affect hearing. Depending on the case, some also have issues with their teeth.
What problems are associated with cleft lip and cleft palate?
Problems with eating, hearing and speech are common in children with clefts. Children may also have issues with their teeth or self-esteem.
Eating problems
With a separation or opening in the palate, food and liquids can pass from the mouth back through the nose. Some babies have difficulty breastfeeding or taking a bottle because they can’t form a good seal around the nipple.
Hearing loss
Children with cleft palate are more prone to fluid buildup in the middle ear (glue ear). If left untreated, this causes hearing loss.
Speech problems
Children with cleft palate may also have trouble speaking. Their voices don’t carry well, sound nasally, and the speech may be difficult to understand. Not all children have these problems, and surgery may fix these problems entirely.
Dental problems
Children with clefts are prone to dental problems like cavities and missing, malformed or displaced teeth.
They may be more prone to defects of the alveolar ridge, the bony upper gum that contains the teeth. A defect in the alveolus can:
- Displace, tip, or rotate permanent teeth.
- Prevent permanent teeth from appearing.
- Prevent the alveolar ridge from forming.
- Cause premature loss of erupting canine and incisor teeth.
Emotional or social problems
Children with clefts may be self-conscious or embarrassed about their appearance, even at a young age. This can cause emotional, social or behavioral problems at school and lead to issues with their confidence.
Who treats children who have cleft lip and palate?
Healthcare providers work together to develop a care plan because of the number of oral health and medical problems associated with a cleft lip or cleft palate. Treatment usually begins in infancy and often continues through early adulthood.
Members of a cleft lip and palate team may include:
- A cleft surgeon to evaluate and perform necessary surgeries on the lip or palate.All cleft surgeons have had extensive training in plastic and reconstructive cleft surgery.
- Pediatrician.
- An orthodontist to straighten and reposition teeth.
- A dentist or pediatric dentist to perform routine dental care
- A prosthodontist to make artificial teeth and dental appliances.
- Speech pathologists to assess speech and feeding problems.
- ENT surgeon
- Oral maxillofacial surgeon.
- Audiologist (a specialist in hearing disorders) to check and monitor hearing.
- Social worker/psychologist to support the family and note any adjustment problems.
- Genetic counselors help parents and adult patients understand the chances of having more children with a cleft palate or cleft lip.
How do doctors fix a cleft lip and cleft palate?
Treating cleft lip and cleft palate depends on the extent of the cleft, the child’s age and other special needs or health conditions. Surgery is performed at a hospital, and the child gets anesthesia so they are asleep during the procedure.
Before lip surgery:
Several techniques can improve the outcomes of cleft lip and palate repairs when used appropriately before surgery. They are non-invasive and dramatically change the shape of the baby’s lip, nose and mouth:
- A lip-taping regimen can narrow the gap in the child’s cleft lip.
- A nasal elevator helps form the correct shape of the baby’s nose.
- A nasal-alveolar molding (NAM) device may be used to help mold the lip tissues into a more favorable position in preparation for lip repair.

Before nasoalveolar molding

Nasoalveolar molding in progress

Before lip surgery

After lip surgery with minimal scar
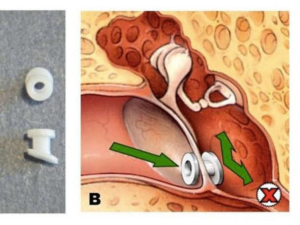
To prevent fluid buildup in the middle ear, children with cleft palate usually need special tubes placed in the eardrums to aid fluid drainage, and their hearing needs checked once a year.
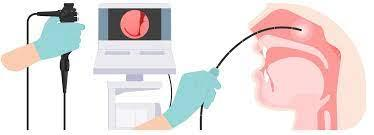
Some children with a cleft palate need further surgeries to help improve their speech. A speech pathologist assesses speech between ages 4 and 5. They may use a nasopharyngeal scope to check the movement of the palate and throat. If surgery is needed to improve speech, this surgery is usually performed around age 5.
Children with a cleft involving the gum line may also need a bone graft when they are between 8 and 12 years of age to fill in the upper gum line so that it can support permanent teeth and stabilize the upper jaw. Due to the cleft and also as a result of multiple surgeries, teeth are usually not in good alignment.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
After 6+ years of age, initial jaw expansion helps create space for bone grafting, thus closing the jaw defect.
{kind=link}
{kind=link}
Once the permanent teeth grow in, a child will often need braces to straighten the teeth and a palate expander to widen the palate.
Additional surgeries could include surgery to:
- Improve the appearance of the lip and nose.
Lip revision and nose surgery are best done once dental correction and jaw surgeries, if needed, have been completed. This gives a stable skeletal foundation for the nose.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Close openings between the mouth and nose.
{kind=link}
{kind=link}
{kind=link}
- Help to breathe.
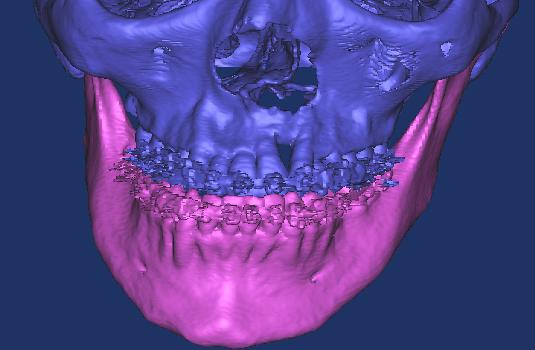
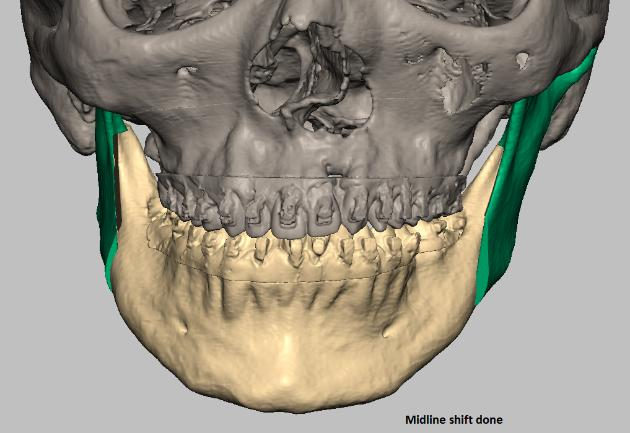
- Stabilize and straighten the jaw.
Jaw surgeries are done after the completion of growth, if the discrepancy between the jaws cannot be corrected by braces alone.
This procedure requires virtual planning and surgery simulation for a good outcome.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Possible risks to surgery include bleeding, infection and damage to nerves, tissues or other structures.